An insight into the real problems that confront thalassemia management.
Since the beginning of this century, the availability of oral chelation therapy has enhanced to opportunity to improve overall survival and quality of life of patients suffering from thalassemia. However, are we adequately monitoring the overall survival associated with management of thalassemia? This is crucial because it may help identify the gaps in the delivery of healthcare to the patients.
We did a preliminary analysis of the survival of the patients who have registered at one of our thalassemia care centres since November 2011.
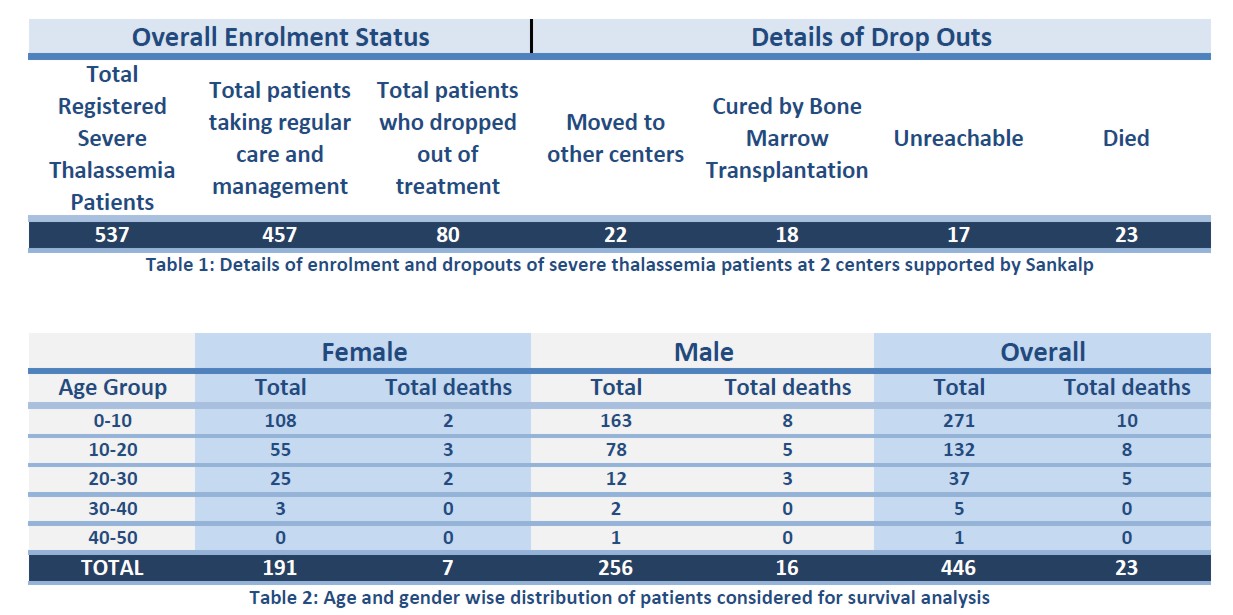
Of the 457 who are taking regular care and management, accurate date of birth was not available for 33 patients and therefore they were excluded from the analysis.
Finally 424 patients who are continuing management at our centres and the 23 who dies in the course of management were selected. Kaplan-Meier survival analysis which is often used to measure the fraction of patients living for a certain amount of time after treatment was done. The figure shows the resultant survival curve.
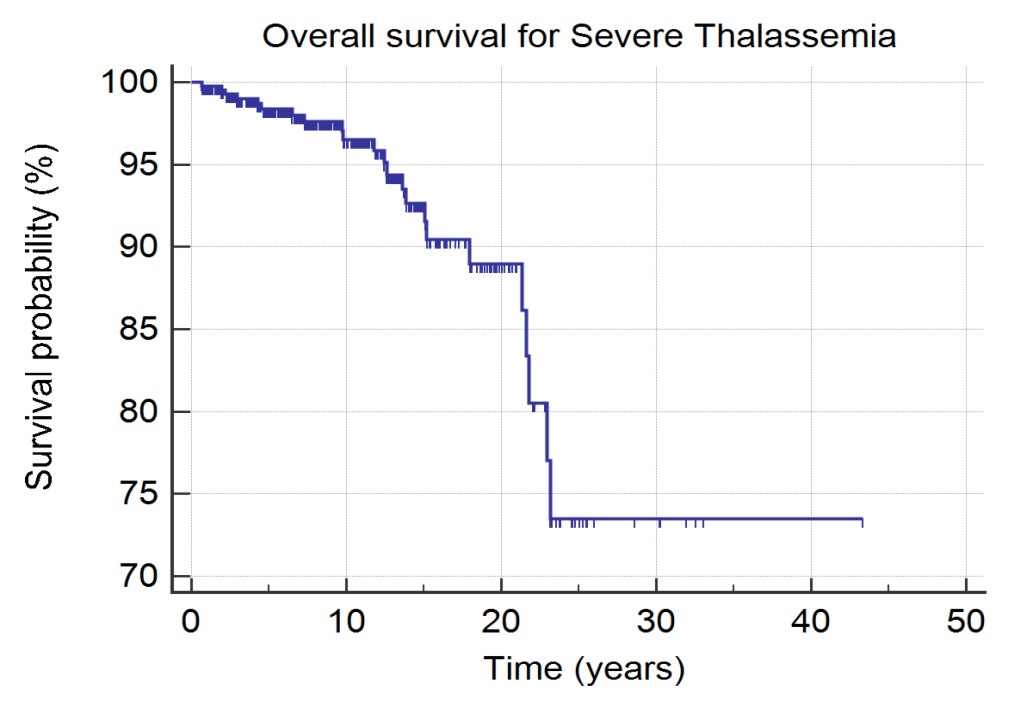
The survival curve suggests that the overall survival at the age of 10 years is 97%. The same drops to 89% by the age of 20 and further down to 73% by the age of 25 years. This information is crucial for us as an organisation to take informed progressive decisions on the roadmap towards management and cure. The survival curve shows the more optimistic of the view as our experience suggests that some of those who are out of contact may have stopped responding to the calls after sudden death of their wards. The other thing to be kept in mind is that most of the individuals started receiving regular chelation therapy only after joining our centres and had been under-transfused and under-chelated at the time of registration.
The few immediate take-aways from the above analysis are as follows:
- A lot of work remains to be done to improve the overall survival of the individuals suffering from thalassemia. In-spite of the better care, there is still significant mortality.
- In our experience problems associated with iron overload, and infections after splenectomy were the major contributors to mortality. Of the 22 patients who died 1 was positive for Hepatitis B, 1 for Hepatitis C and 1 for HIV, however, only 1 death happened because of reasons that can be related to transfusion transmitted infections. Ensuring adequate chelation, monitoring of cardiac complications and early management and avoiding splenctomy as much as possible are some of the key areas of focus. Of-course these are issues directly related to survival alone and more interventions are needed to restore the normalcy of life for these patients.
- As of now, the overall survival associated with thalassemia management does not compare favourably with the overall survival expected with bone marrow transplantation from fully matched sibling donors which upwards from 90%. Therefore, each child who has a potential for cure must be offered the option.
These are early findings. We are happy to collaborate with other organizations who may want involve in survival analysis for larger patient groups.